THE HALO FOR CHILDREN WITH DWARFISM
"A halo is not a barrel of fun, but you learn to make the best of the situation and somehow, life returns to normal."
|
|
|
|
Some children with dwarfism -- the term LP (little person) is also used here -- need a halo because they require a fusion of their cervical (neck) vertebrae because of instability and/or dislocation of the cervical vertebrae. Halos are also sometimes worn by LP children who require a fusion of their upper thoracic vertebrae (top part of the spine). If your LP child's doctor has told you that a halo is in your child's future, through to the generosity of the families who provided information for this website, hopefully, you will find some of the answers to your questions here. You will see some of their children's sweet faces throughout this website. This website is not meant to be a substitute for a doctor's care -- your child's doctor will give you the best counsel.
The halo is a rather gruesome looking "gizmo". It does not, however, hurt to wear one and most children get used to it within a few days. Truthfully, the halo will be more difficult for you as a parent than it will be for your child. Seeing your child's darling face in the halo is an experience never forgotten by parents. Fortunately, you will also remember your child's smiles while wearing the halo and what a trouper your child was through the entire experience!
Preparing for Surgery
The first person you have to prepare for this surgery is yourself. That you are here at this website says that you are already well on your way to being prepared. It is suggested that parents think long and hard before surgery, getting as much of their own angst out of the way as possible. Using this method, chances are that when surgery time comes, you will be very calm. A calm parent makes for a calm child -- and a calm child will have an easier time with the whole surgery scenario.
 Some
of what you read (and see) here at this website might seem overwhelming, but
keep in mind that you CAN do this -- and your child definitely can! A positive
attitude goes a long way towards helping your child. You'll feel anxious
at times, but you can't allow your child to see this. While smiles aren't
possible all of the time, at least a matter-of-fact attitude will be helpful.
Many, many LP children and their families have been through the halo experience
and come out on the other side with a positive outlook. Children are extremely
resilient. Your child, no matter how young, is going to amaze you!!!!
Some
of what you read (and see) here at this website might seem overwhelming, but
keep in mind that you CAN do this -- and your child definitely can! A positive
attitude goes a long way towards helping your child. You'll feel anxious
at times, but you can't allow your child to see this. While smiles aren't
possible all of the time, at least a matter-of-fact attitude will be helpful.
Many, many LP children and their families have been through the halo experience
and come out on the other side with a positive outlook. Children are extremely
resilient. Your child, no matter how young, is going to amaze you!!!!
What you tell your child about this surgery and the halo depends on the child's age. For example, the child can be told, "The doctor will be making your neck stronger. First you'll go to sleep and won't feel him working on it. When you wake up, you'll be wearing a hard vest with bars that hold your head still." When discussing the procedure, it is important to use a calm, reassuring tone of voice. It is also helpful to show pictures of what the halo looks like. It is not helpful to go into too much detail because the child will not comprehend it. However, not explaining anything will result in the child being more frightened.
Because older children want more information, it is best to be as straightforward as possible in explaining things, without telling your child unnecessary information that would only serve to worry him/her. Below is an actual conversation that took place between a 9 year old boy and his parent before he had both a cervical fusion and an upper thoracic fusion...
"After
you go to sleep, the doctors will put your halo on so that it will hold your
neck still during the surgery. Next, the doctor will do the fusion part of the
surgery."
"What does fusion mean?"
"A fusion is what happens when you take something that has many pieces
and turn it into one solid piece. You kind of glue them altogether, so they
become stronger. With your surgery, the doctor is going to fuse your vertebrae
(the bony bumps in your spine) together so they can't keep bending and causing
your kyphosis and scoliosis (curves in your spine) to get worse."
"How will he do the fusion?"
"First, he'll take a little bit of bone from your hip to use as the "glue"
for the fusion. Then, he will carefully put the vertebrae in a straighter line,
and put the "bone glue" from your hip between the vertebrae. To help
everything stay in place, he'll put two long metal rods on either side of your
spine, and some little screws will go in different places. All together, the
rods and screws will help the spine stay straight while the "bone glue"
turns hard. Once the "bone glue" hardens-and that will take many months-
the fusion will be called solid. Your spine will not be able to curve anymore
after it is fused because it will be one solid, strong piece of bone."
"How will they know when
my fusion is solid?"
"Every few weeks, the doctor will want to see x-rays of your spine. When
the "bone glue" between the vertebrae looks bright white on the x-ray
pictures, that will mean the fusion has become solid."
"So why do I have to wear
a halo?"
"The halo will hold your neck and back completely still while your fusion
is healing. It is very important for your spine to be totally still after surgery
because too much movement could injure it and cause it not to heal right. Think
of the halo like a cast for your neck and back, only better because it's lighter
and not as hot and itchy as a real cast."
"Will the halo hurt?"
"It will probably feel weird and hurt a little at first, but you'll be
able to take pain medicine if you need it. Then, in a few weeks, you'll be used
to the halo. In fact, I bet you'll feel like playing again sooner than you think.
We can even decorate the halo with cool stickers if you like."
"And when I get it off, can
we have a party?"
"ABSOLUTELY!"
Your child's doctor will give you the particulars about your child's surgery and will also tell you how long it will all take. Just in case it isn't mentioned, you should be prepared for your child's face to be very swollen after surgery. This swelling goes down within a few days, but it is usually a shock for parents, even when they know about it ahead of time.
The Halo
 Today's
halos, as pictured in the photobar above and in the photo on the left, are made
of titanium. The halo bars will be attached to a fleece-lined vest or
a plastic brace jacket or a plaster torso cast. Each doctor has his/her
own preferred method, so this is a question you want to ask beforehand.
Today's
halos, as pictured in the photobar above and in the photo on the left, are made
of titanium. The halo bars will be attached to a fleece-lined vest or
a plastic brace jacket or a plaster torso cast. Each doctor has his/her
own preferred method, so this is a question you want to ask beforehand.
Because of the lighter weight of today's halos, your child will probably be allowed to sit up after a certain amount of time. Your doctor will tell you the timetable for your particular child.
Your child might also be allowed to stand, walk with a walker, or walk independently. Again, the doctor has the final say as to if and/or when this is allowed to happen.
How long your child will need to wear the halo is also something your child's doctor will tell you. Some need them for 3 months, whereas others need them for 6 months or longer.
Just for fun, you can decorate your child's halo! Stickers, ribbon, beads, whatever strikes your child's fancy, as long as the pins themselves are not covered. You can see some decorative examples in the photobar at the top of the page.
Halo Ring, Pins, and Body Jacket/Vest
The halo ring is attached to the halo rods. The ring is held steady on the head using "pins". These pins do not penetrate the skull itself. There will be at least 4 pins, and sometimes as many as 8 pins. Religious pin care is essential to avoid infection. Pin care is discussed below. Pins can also become loose and sometimes one or more of them need to be replaced. Ask your child's doctor about the signs that you should watch for, in terms of infection and loosening of the pins.
The photo on the left, below, shows a child immediately after surgery. This particular child has had a trach/vent almost from birth -- this is not part of the usual halo experience. Also notice that this child's halo rod brackets are attached to a plastic torso jacket. This is just one setup. The photo on the right, below, shows a child wearing a fleece-lined vest. Your child's doctor will tell you what he usually prefers to use, so it's a question worth asking. If the doctor mainly uses the fleece-lined vest, let the doctor know this ahead of time if your child is allergic to wool since synthetic liners are available.
 |
 |
Pin Care
The halo pins must be religiously cleaned to avoid infection. Individually wrapped, sterile 6-inch cotton swabs can be purchased cheaply at your local medical supply store. These swabs come with the cotton on one or both ends. Because you will use a lot of these while your child wears the halo, the type with cotton on both ends are more useful (but not imperative).
A common solution used for cleaning halo pins is sterile saline. Your child's doctor will give you instructions to get you started, including telling you which solution(s) he/she prefers for his/her patients.
 No
matter which solution(s) your child's doctor recommends, clean one pin at a
time, using one swab end for each pin. To avoid cross-contamination, do not
double-dip a swab into any solution -- instead, use a new swab if a pin needs
further cleaning. Pin cleaning must be done according to the doctor's
schedule choice (once a day, once every two days, etc.) -- no excuses.
No
matter which solution(s) your child's doctor recommends, clean one pin at a
time, using one swab end for each pin. To avoid cross-contamination, do not
double-dip a swab into any solution -- instead, use a new swab if a pin needs
further cleaning. Pin cleaning must be done according to the doctor's
schedule choice (once a day, once every two days, etc.) -- no excuses.
Inspect pin sites carefully for early signs and symptoms of infection, including fever over 101, redness, tenderness, drainage, pain and swelling. Do not hesitate to call your child's doctor if you suspect pin infection! If you notice head or pin movement, again, call your child's doctor.
Sleeping
At first, your child will not be accustomed to sleeping with his/her head suspended in the halo. Putting a small, very soft (thin and floppy) pillow, a rolled towel or pillowcase between your child's head and the back of the neck (when lying on the back) or next to the cheek (when lying on the side) will help your child feel more normal. It is important that whatever you use merely contacts your child's skin and does not apply pressure.
Your child may or may not be able to roll over while in the halo. If your child cannot accomplish this, some parents set up a bed (or mattress) in their room for the child or use a baby monitor in the child's room. Ask your child's doctor how often your child's position should be changed while sleeping. An alarm clock, if necessary, is a helpful alert for yourself to help your child to change position.
Hair Washing
Your child's hair will be cut/shaved in back in the incision area in the operating room. Still, it has been suggested that you get your child's hair cut short since that makes hair washing easier later on. While little girls have worn halos with long hair, a shorter hairstyle, preferably with no bangs, is definitely easier and makes hair washing less of a chore.
Hair washing is an essential part of keeping the pins at the back of the head in good shape. While most families are given dry shampoo in the hospital, this can only work for so long. By the time your child comes home, he/she will probably need a good hair washing.
There are many approaches to washing hair while in a halo. Because LP children are smaller, usually hair washing can be done by laying the child on your kitchen counter, protecting the vest/jacket/cast with plastic and lots of toweling. The vest/jacket/cast cannot get wet! All of this might seem awkward at first, but it will get easier.
Bathing
Sponge baths are the main source of bathing, using minimal amounts of soap and water. It has been suggested by experienced parents that Johnson's Baby Bath is good since it rinses more easily and more thoroughly.
Once your child is sitting up, you can bathe his/her lower half -- not getting the vest/jacket/cast wet -- in your kitchen sink, with the child sitting on the edge of the sink. For a larger LP child, having the child sit on a plastic stool in the tub will work. No matter which technique you choose, make sure that you are right there at all times since the child could lose his/her balance. Falling is NOT good, needless to say.
Itching
 Due
to dry skin or even the drugs your child might take for post-op pain, itching
can happen at any time during the halo experience. Using the witch hazel
techniques mentioned above will help a lot, as will knocking on the vest/jacket/cast.
You can also run a hair dryer on the "cool" setting, shooting inside
the vest/jacket/cast. If your child needs more than that, talk to the
doctor about changing drugs and/or using something like Benedryl.
Due
to dry skin or even the drugs your child might take for post-op pain, itching
can happen at any time during the halo experience. Using the witch hazel
techniques mentioned above will help a lot, as will knocking on the vest/jacket/cast.
You can also run a hair dryer on the "cool" setting, shooting inside
the vest/jacket/cast. If your child needs more than that, talk to the
doctor about changing drugs and/or using something like Benedryl.
Sitting
Although today's halos are more lightweight, your child will still be somewhat top heavy. The size of the child and arm length a lot to do with how much balance that child will have while sitting in a halo (or standing if and/or when the time comes and the doctor approves). A smaller LP child will be more top heavy than a taller, heavier LP child.
 Providing
side-to-side sitting support is a good idea, especially in the beginning. Many
families rent a wheelchair for both inside the house and outside traveling,
but often a large stroller will do for a younger, smaller child.
Providing
side-to-side sitting support is a good idea, especially in the beginning. Many
families rent a wheelchair for both inside the house and outside traveling,
but often a large stroller will do for a younger, smaller child.
For a smaller LP child or one with shorter arms, you also want to avoid a lot of bending forward to grab toys, food, books, etc. since that can make a child with otherwise good balance lose it and fall forward. A reacher is helpful to bring things closer to the child -- this reacher can be as simple as a plastic beach rake (sample on the right).
![]() Experienced
families suggest that even when your child can sit up safely on his/her own,
either with a couch as a back rest or all on their own, that you keep a "safety
pillow" closeby, for emergency rest breaks.
Experienced
families suggest that even when your child can sit up safely on his/her own,
either with a couch as a back rest or all on their own, that you keep a "safety
pillow" closeby, for emergency rest breaks.
If a child is lying down and wants to sit up, encourage your child to go onto his/her side first and then push up with his/her arms. Sitting straight up from a lying down position can be too much of a strain on the halo pins. Click on the photo on the left to see how this transition can be made safely.
Falling in a halo is not a good thing -- but if your child does fall, keep a close watch on any repercussions of that fall. Definitely feel free to contact your child's doctor at any time that you have questions. Keep in mind that the doctor works for your child, not the other way around.
Eating, Playing, and School
 Because
your child will be unable to look down -- practice this yourself to see the
effect of not being able to bend your neck -- having food, toys, and writing
and art supplies on a surface that's a tad higher than mid-chest height allows
easy access for eating and playing while seated. The length of the arms
must, of course, also be taken into account.
Because
your child will be unable to look down -- practice this yourself to see the
effect of not being able to bend your neck -- having food, toys, and writing
and art supplies on a surface that's a tad higher than mid-chest height allows
easy access for eating and playing while seated. The length of the arms
must, of course, also be taken into account.
If your child has mid-chest halo brackets, reach can be accomplished both outside the bars or inside the bars -- or as the photo on the right shows, sometimes all at once!
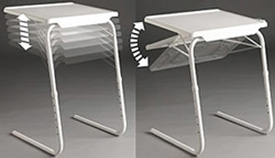
Providing a slanted easel-like surface is also good for some things -- writing, art work, etc. You will have to play around with heights and surfaces to find out which one works best for whichever activity your child is doing at the time. Play tables or breakfast trays can provide the extra height. The legs on play tables can be cut down to the appropriate height -- once you figure out what that height is, of course. Some samples are shown below, including a play table with cut-down legs. The other table shown below is a Table-Mate II. This table is adjustable up and down and the top can tilt as well. While there is no guarantee that this table will be available for purchase forever, it might give some families who are handy an idea of how to make something similar.
 |
|
 |
During mealtimes and snacks, experienced parents agree that an eating cloth or bib is a must! Again, this has to do with your child not being able to look down. The travel path from the plate to the mouth can get messy without an eating cloth or bib.
 Playtime
activities will be mostly sedentary ones, but if they are interesting enough,
your child won't mind. Video and PC games were practically invented for
children in halos! For board games, give your child a reacher (or dowel)
to push the pieces around the game board, so that your child won't be tempted
to bend to far forward and lose balance. Unless the activities are rather
sedentary, check with your child's doctor before allowing much outside playtime.
Playtime
activities will be mostly sedentary ones, but if they are interesting enough,
your child won't mind. Video and PC games were practically invented for
children in halos! For board games, give your child a reacher (or dowel)
to push the pieces around the game board, so that your child won't be tempted
to bend to far forward and lose balance. Unless the activities are rather
sedentary, check with your child's doctor before allowing much outside playtime.
 By
all means continue to have your child's friends and relatives over to visit
at your house. Children, even very young ones, are mostly fascinated by the
halo at first -- "like a rocket ship", said one 5 year old friend
-- but they get over it quickly. One family had a Girl Scout troop come to their
house, a few girls at a time, for a few times each week to play with their toddler-age
child while he was in his halo. Not only did their child love these visits
-- music, stories, skits, etc. -- but the scouts also loved this activity and
even won badges for it.
By
all means continue to have your child's friends and relatives over to visit
at your house. Children, even very young ones, are mostly fascinated by the
halo at first -- "like a rocket ship", said one 5 year old friend
-- but they get over it quickly. One family had a Girl Scout troop come to their
house, a few girls at a time, for a few times each week to play with their toddler-age
child while he was in his halo. Not only did their child love these visits
-- music, stories, skits, etc. -- but the scouts also loved this activity and
even won badges for it.
 Your
adult relatives will have a much harder time dealing with seeing your child
in the halo. Feel free to tell them that if they start to get upset, they
should leave the room until they get themselves together. This is about
your child's feelings, not the adult's feelings.
Your
adult relatives will have a much harder time dealing with seeing your child
in the halo. Feel free to tell them that if they start to get upset, they
should leave the room until they get themselves together. This is about
your child's feelings, not the adult's feelings.
 At
some point, your child will begin to feel noticeably better and will want to
do more. In keeping with your doctor's orders, it is suggested that you
not allow your child to do anything unless you have permission.
At
some point, your child will begin to feel noticeably better and will want to
do more. In keeping with your doctor's orders, it is suggested that you
not allow your child to do anything unless you have permission.
In time, your child will be able to keep occupied with many of the usual activities he/she has always enjoyed. The only exceptions are the ones requiring walking, running, lifting and jumping. Even if and/or when a child is allowed to walk on their own (or with a walker), parental supervision still needs to be constant.
Some children are able to continue to attend school while wearing a halo, but only if they have a wheelchair, a one-on-one aide, and a setup that will allow them to read and write conveniently. Your child's school can also arrange for a home school teacher to come to your home. Most children who have used this home school teacher arrangement end up being ahead of their class when it comes to schoolwork. If you choose to do this, make arrangements through your school principal before your child has his surgery.
Adapting
a Shirt for a Halo
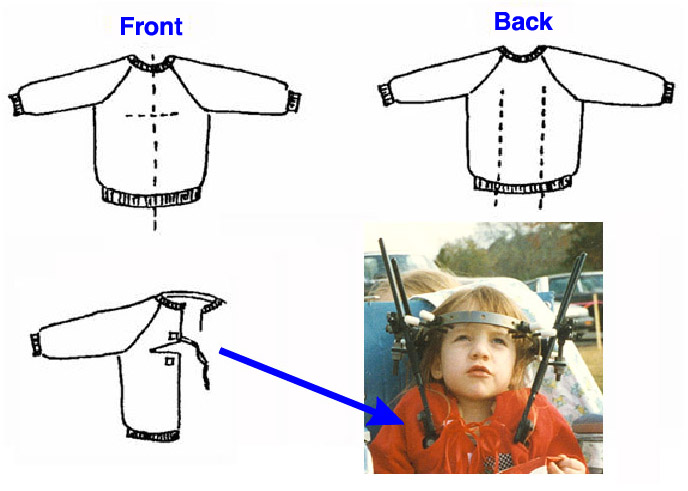
 Lay
the shirt over the child's front and eyeball or mark where the top of the
halo bars are attached to the cast. Make a slit from the hem of the teeshirt
to the top of the halo bar -- one slit for each bar.
Lay
the shirt over the child's front and eyeball or mark where the top of the
halo bars are attached to the cast. Make a slit from the hem of the teeshirt
to the top of the halo bar -- one slit for each bar. Your
child will need something to wear home from the hospital. It is very helpful
to make a few halo teeshirts at home and bring them with you to the hospital.
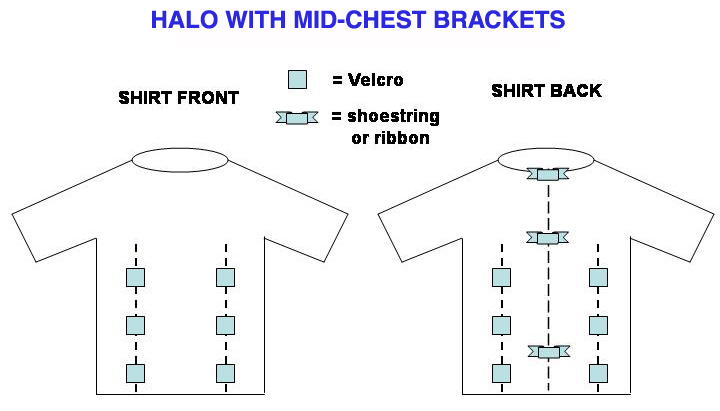
For halos with mid-chest brackets, follow the proportions of the slits
in the teeshirt diagrams below (see sample, left) -- you can always cut
the slits higher at the hospital if you need more room than you thought for
the halo brackets. Slits for both front and back brackets can be cut at
the same time. Add velcro buttons, shoestring or ribbon ties before you leave
home, or use safety pins (until you return home).
Your
child will need something to wear home from the hospital. It is very helpful
to make a few halo teeshirts at home and bring them with you to the hospital.
For halos with mid-chest brackets, follow the proportions of the slits
in the teeshirt diagrams below (see sample, left) -- you can always cut
the slits higher at the hospital if you need more room than you thought for
the halo brackets. Slits for both front and back brackets can be cut at
the same time. Add velcro buttons, shoestring or ribbon ties before you leave
home, or use safety pins (until you return home).
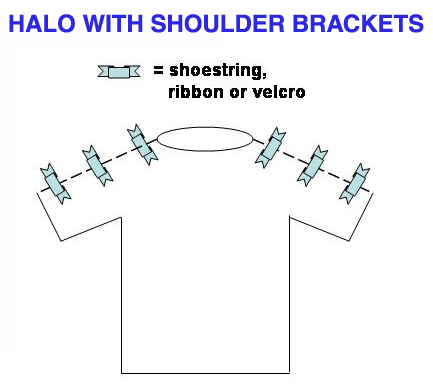
For a halo with shoulder brackets, in cold weather the zip-front "hoodie" above will work for the trip home. In warmer weather, or for under the zip-front jacket, a tank top with velcro at the shoulder seams can be worn.
Because you will have already asked your child's doctor which type of halo he/she uses, you will know which kind of halo shirt to make -- and if not, bring at least the zip-front jacket and some larger teeshirts that can be adapted at the hospital.
 |
|
 |
|
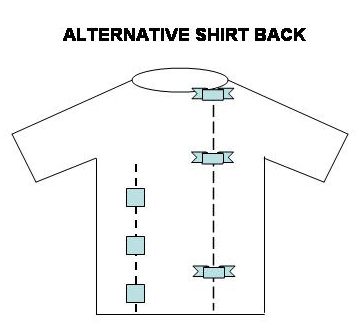
An alternative idea for halos with mid-chest brackets is shown below. Notice the innovative slit on the front of this child's jacket.
Traveling, Carseats, and Strollers
Your child's doctor will advise you on how often your child is allowed to ride in a car. This advice is very important, so make sure to get clear instructions before your child leaves the hospital.
For the youngest halo patients who still need a rear-facing carseat, finding a carseat to accommodate the width of the top of the halo can be a challenge. You want to look for one that is rather wide at the top of the seat, with no close-in wings. The photos below show such a carseat -- this one was made by Evenflo.
Two of the pictures below show the rear of the car seat. Figure 1 illustrates how the straps can be removed and slipped back onto the bracket. Figure 2, the photo with the pole through the back, is meant to show this car seat can be reattached to the bracket in another location, making the straps short enough to provide the snug fit required for safe travel.
Any rear facing car seat will work for many of the kids that can still rear face. This Evenflo carseat is advantageous over other rear facing seats in the case of a very small child, mainly because this carseat has a second place where the strap could be attached to the bracket. The straps have to be loosened and reattached every time a child uses this carseat. Experienced parents say that this sounds much more difficult than it actually is and takes no longer to do than using the restraint in a conventional manner. It just takes a little practice.
 |
 |
 |
|
Evenflo
Infant Carseat
|
FIGURE
1
|
FIGURE
2
|
For older children, an Evenflo booster seat can be the answer to car safety. The Evenflo booster seat shown below has multiple slots for strap attachment, and process for getting the straps loosened from the bracket and then refastened works similar to the rear-facing infant seat described above.
 |
 |
 |
|
Evenflo
Booster Seat
|
Straps
Detach via Rear Bracket
|
Straps
Loose
|
 |
 |
|
Straps
Attached to Rear Bracket
|
Straps
go through middle slot for this child.
|
While older children can use a wheelchair to get around both inside and outside the house, younger smaller children can usually get away with using a stroller. Not just any stroller, but one that, like the carseat above, has adequate room to accommodate the width of the top of the halo. One such stroller is the Graco Literider, shown below. Aside from the top width of this stroller, the straps are easily threaded through the halo so that the safety features of the harness can be maintained.
 |
 |
 |
Halo Removal and Its Aftermath
The halo removal process will not be pleasant. Fortunately, it only takes a few minutes and then it's GONE!! Some doctors will use anesthesia or sedation for young patients, but most children are awake and aware when their halo is removed. Parents are sometimes asked to help the doctor, but if you are not comfortable doing so, feel free to speak up.
The pin holes start to close almost immediately and are looking pretty good within days. There will always be scars at the pin sites, but once the pin sites have healed, with a little Mederma (available in most grocery stores and pharmacies), you can lessen the look of them. Do not put Mederma on the pin sites until the holes have healed or until your child's doctor tells you that it's okay to do so.
Your doctor will most likely have your child wear some sort of neck restraint after halo removal. The doctor will also advise you on how long your child's individual needs will require use of the neck restraint. Some children will continue to wear their neck restraint while traveling in a car for as long as a year after the halo comes off. There are several types of neck restraints, a few of which are shown below.
 |
 |
 |
 |
|
Aspen
Cervical Collar
|
Miami
Jr Cervical Collar
|
Custom
Neck Brace
|
Soft
Cervical Collar
|
Lining the chin part of any neck brace with moleskin helps to keep skin irritation down. Some of the neck braces come with replacement liners. Experienced parents suggest that you get 2-3 extra liners.
FINISHED WITH MY HALO, BUT I'M STILL AN ANGEL...
 |
 |
 |
 |
Acknowledgments
Many thanks to the families who helped this website become a reality. Special thanks to the families of Andrew, Cailie, Elizabeth, Hannah, Sara, and Stefan for their invaluable input in the making of this website. It is their hope that other families will find useful information here to make the halo experience less daunting. Below is a list of contacts for anyone interested in hearing more specific experience stories. It is suggested that when writing to any of these contacts that your subject line contain the word "Halo".
|
Parent: Denise
(Deniseaguiar@yahoo.com) |
Parent: Kristin
(lindnerk21@hotmail.com) Child: Hannah, Campomelic Dysplasia, age 4 in halo |
| Parent: Jayna
(jaynamiller@columbus.rr.com) Child: Andrew, Campomelic Dysplasia, age 9 in halo |
Parent: Marj
(marji.mcilvaine@gmail.com) Child: Elizabeth, SED, age 4 in halo |
| Parent: Vita
(vitagagne@yahoo.com) Child: Stefan, Diastrophic Dysplasia, age 3.75 in halo |
References
A printable PDF version of this website is available: The-Halo-for-Children-with-Dwarfism.pdf (9Mb)
This Web site and all its contents, including this home page and all pages at
this site that are linked to it, are copyright © 2014 by Vita Gagne.
In addition, all photographs on this Web site are the copyrighted property of
the webmaster or the individuals pictured, and have been posted with their permission.
All rights reserved. To obtain legal copies of these photographs for any purpose
whatsoever, contact Vita Gagne
Last Updated by Vita Gagne, 02/28/2011